โครงการสร้างเสริมภูมิคุ้มกันโรค
Expanded Programme on Immunization (EPI)
ประเทศไทย พ.ศ. 2569
Nutthawat Nongnual, M.D.
Department of Pediatrics,
King Chulalongkorn Memorial Hospital
Routine Childhood Immunization Schedule (NIP Thailand 2026)
Page 1 — Birth to 12 months
| Age | Vaccine | Dose | Route | Site / Note |
|---|---|---|---|---|
| At Birth | BCG | 0.1 mL | ID | Left shoulder |
| At Birth | Hepatitis B (HB1) | 0.5 mL | IM | Left anterolateral thigh |
| 1 Month | Hepatitis B (HB2) | 0.5 mL | IM | Only if maternal HBsAg positive |
| 2 Months | DTPw-HB-Hib1 | 0.5 mL | IM | Anterolateral thigh |
| 2 Months | IPV1 | 0.5 mL | IM | Separate injection site |
| 2 Months | Rotavirus (Rota1) | Oral | PO | Oral drops |
| 2 Months | PCV1 | 0.5 mL | IM | Anterolateral thigh |
| 4 Months | DTPw-HB-Hib2 | 0.5 mL | IM | Anterolateral thigh |
| 4 Months | IPV2 | 0.5 mL | IM | Separate injection site |
| 4 Months | Rotavirus (Rota2) | Oral | PO | Oral drops |
| 4 Months | PCV2 | 0.5 mL | IM | Anterolateral thigh |
| 6 Months | DTPw-HB-Hib3 | 0.5 mL | IM | Anterolateral thigh |
| 6 Months | OPV1 | 2 drops | PO | Oral drops |
| 6 Months | Rotavirus (Rota3) | Oral | PO | Only for 3-dose vaccine |
| 9–12 Months | MMR1 | 0.5 mL | SC | Left deltoid |
| 9–12 Months | Live JE (LAJE1) | 0.5 mL | SC | Right deltoid |
| 12 Months | PCV3 booster | 0.5 mL | IM | Anterolateral thigh |
Routine Childhood Immunization Schedule (NIP Thailand 2026)
Page 2 — 18 months to adolescence
| Age | Vaccine | Dose | Route | Site / Note |
|---|---|---|---|---|
| 18 Months | DTP4 booster | 0.5 mL | IM | Thigh or deltoid |
| 18 Months | OPV2 | 2 drops | PO | Oral drops |
| 18 Months | MMR2 | 0.5 mL | SC | Deltoid |
| 2–2.5 Years | Live JE (LAJE2) | 0.5 mL | SC | Upper arm deltoid |
| 4–6 Years | DTP5 booster | 0.5 mL | IM | Deltoid |
| 4–6 Years | OPV3 | 2 drops | PO | Oral drops |
| Grade 5 (11–12 Years) | HPV | 0.5 mL | IM | Deltoid; school-based campaign |
| Grade 6 (12 Years) | dT | 0.5 mL | IM | Deltoid; repeat every 10 years |
BCG Vaccine & Complications Management
Mechanism & Routine Administration
Live-attenuated Vaccine: Live-attenuated BCG vaccine protects against severe tuberculosis in infants, including disseminated TB and tuberculous meningitis.
Dose & Route: 0.1 mL intradermally (ID) at the left shoulder/upper arm. Administered strictly Intradermally (ID) at the left deltoid (outer upper arm).
BCG Complications & Management Guidelines
Ipsilateral axillary or supraclavicular lymph node swelling (>1.5 cm) on the injected side.
Non-suppurative: Conservative observation. Usually resolves spontaneously over weeks.
Suppurative (Fluctuant/Threatening rupture): Needle aspiration is preferred to prevent sinus formation. Avoid incision & drainage (I&D).
Large ulceration (>10 mm) or cold abscess. Often due to deep (subcutaneous) injection. Manage conservatively; do not apply topical antibiotics or excise.
Systemic infection in immunodeficient hosts (SCID, advanced HIV). Requires systemic anti-TB therapy. Note: M. bovis BCG is intrinsically resistant to Pyrazinamide (PZA).
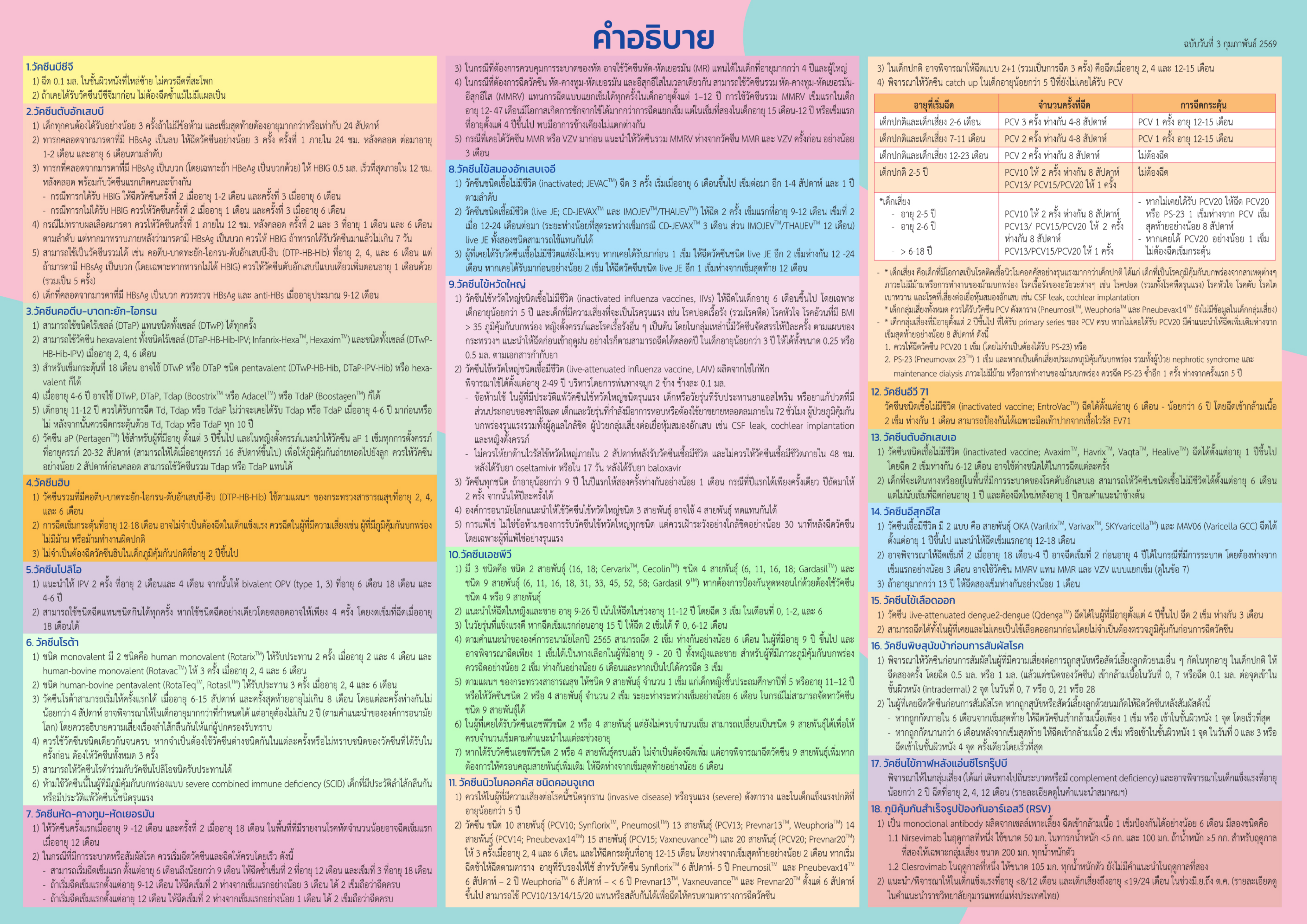
คำอธิบายเต็ม: BCG
1) ฉีด 0.1 มล. ในชั้นผิวหนังที่ไหล่ซ้าย ไม่ควรฉีดที่สะโพก
2) ถ้าเคยได้รับวัคซีนบีซีจีมาก่อน ไม่ต้องฉีดซ้ำแม้ไม่มีแผลเป็น
Hepatitis B Vaccine (HepB - Birth Dose)
Subunit Vaccine & Core Timeline
Recombinant Subunit Vaccine: Uses recombinant HBsAg to prevent vertical and horizontal transmission of Hepatitis B virus (which leads to chronic hepatitis, cirrhosis, and hepatocellular carcinoma).
Standard Schedule: 0.5 mL Intramuscular (IM) injection at the right anterolateral thigh (Vastus Lateralis) within 24 hours of birth.
Maternal HBsAg Carrier Management
If the mother is HBsAg positive:
1. Administer HBIG 0.5 mL IM + HB1 0.5 mL IM at separate thighs within 12 hours of birth.
2. Administer monovalent HB2 at 1 month. Follow with routine pentavalent (DTP-HB-Hib) at 2, 4, 6M (total 5 HB doses).
3. Test for HBsAg and anti-HBs at 9-12 months to verify protection status.
คำอธิบายเต็ม: Hepatitis B (HepB)
1) เด็กทุกคนต้องได้รับอย่างน้อย 3 ครั้งถ้าไม่มีข้อห้าม และเข็มสุดท้ายต้องอายุมากกว่าหรือเท่ากับ 24 สัปดาห์
2) ทารกจากมารดา HBsAg ลบ: เข็มที่ 1 ภายใน 24 ชม. หลังคลอด ต่อมาอายุ 1–2 เดือน และ 6 เดือน
3) ทารกจากมารดา HBsAg บวก โดยเฉพาะ HBeAg บวก: ให้ HBIG 0.5 มล. เร็วที่สุดภายใน 12 ชม. พร้อมวัคซีนแรกเกิดคนละข้าง
- ได้ HBIG: เข็มที่ 2 อายุ 1–2 เดือน และเข็มที่ 3 อายุ 6 เดือน
- ไม่ได้ HBIG: เข็มที่ 2 อายุ 1 เดือน และเข็มที่ 3 อายุ 6 เดือน
4) หากไม่ทราบผลเลือดมารดา ให้เข็มแรกภายใน 12 ชม. และเข็มที่ 2, 3 อายุ 1 และ 6 เดือน
5) ใช้เป็นวัคซีนรวม DTP-HB-Hib ที่อายุ 2, 4, 6 เดือนได้
6) เด็กจากมารดา HBsAg บวกควรตรวจ HBsAg และ anti-HBs อายุประมาณ 9–12 เดือน
DTwP-HB-Hib
Indications & Schedule
Combined Vaccine: Protects against Diphtheria, Tetanus, whole-cell Pertussis, Hepatitis B, and Haemophilus influenzae type b (Hib) in a single injection.
Timeline: 0.5 mL Intramuscular (IM) injection at the Vastus Lateralis (anterolateral thigh) at 2, 4, and 6 months of age.
Reactogenicity & Clinical Cautions
Local & Systemic Reactions: High rate of local pain, redness, swelling, and moderate-to-high fever within 24-48 hours because wP vaccines generally have higher reactogenicity. Manage with supportive cool compresses and Paracetamol.
Contraindication: Encephalopathy within 7 days after a previous pertussis-containing dose. Seizure history alone is not equivalent; defer vaccination for an unstable neurologic condition until evaluated.
คำอธิบายเต็ม: คอตีบ–บาดทะยัก–ไอกรน (DTP/DTaP/Tdap)
1) ใช้ชนิดไร้เซลล์ (DTaP) แทนชนิดทั้งเซลล์ (DTwP) ได้ทุกครั้ง
2) ใช้ hexavalent DTaP-HB-Hib-IPV หรือ DTwP-HB-Hib-IPV อายุ 2, 4, 6 เดือน
3) เข็มกระตุ้น 18 เดือน ใช้ DTwP หรือ DTaP pentavalent หรือ hexavalent ได้
4) อายุ 4–6 ปี ใช้ DTwP, DTaP, Tdap หรือ TdaP ได้
5) อายุ 11–12 ปี ควรได้ Td, Tdap หรือ TdaP แล้วกระตุ้นทุก 10 ปี
6) หญิงตั้งครรภ์ควรได้ aP/Tdap 1 เข็มทุกการตั้งครรภ์ อายุครรภ์ 20–32 สัปดาห์
Pertussis Component Analysis: wP vs. aP Comparison
Whole-cell Pertussis (wP) - Public Sector
Composition: Uses killed whole-cell bacteria, preserving all structural antigens and endotoxin Lipid A.
Pros: Induces robust cell-mediated immunity (Th1/Th17 pathway), providing long-lasting protection and herd immunity.
Cons: Higher rates of local reactogenicity and fever.
Acellular Pertussis (aP) - Private Sector
Composition: Contains purified, isolated bacterial antigens (PT, FHA, Pertactin).
Pros: Significantly lower reactogenicity (fever and local swelling reduced by 70-80%). Highly preferred in private practices.
Cons: Faster waning immunity (shorter duration of protection) compared to wP.
คำอธิบายเต็ม: เปรียบเทียบ wP และ aP
ชนิดทั้งเซลล์ (wP) และไร้เซลล์ (aP) ใช้ตามข้อบ่งชี้และผลิตภัณฑ์ หากขาดช่วงไม่ต้องเริ่มใหม่ ให้ฉีดเข็มที่เหลือตามระยะห่างขั้นต่ำ
Haemophilus influenzae type b Vaccine (Hib)
Pathogen & Rationale
Hib Conjugate Vaccine: Prevents bacterial meningitis, sepsis, pneumonia, and epiglottitis caused by Haemophilus influenzae type b, particularly in children under 5.
EPI Delivery: Provided as part of the pentavalent (DTPw-HB-Hib) vaccine at 2, 4, and 6 months.
Special Cohorts & Catch-up
At-risk cohorts: A booster at 12–18 months may be needed for children with immunodeficiency, asplenia, or splenic dysfunction; it may not be necessary for healthy children.
Reactogenicity is generally mild, consisting of brief localized pain or low-grade fever.
คำอธิบายเต็ม: Hib
1) วัคซีนรวม DTP-HB-Hib ใช้ตามแผนกระทรวงสาธารณสุข อายุ 2, 4 และ 6 เดือน
2) เข็มกระตุ้นอายุ 12–18 เดือนอาจไม่จำเป็นในเด็กแข็งแรง แต่ควรฉีดในเด็กเสี่ยง เช่น ภูมิคุ้มกันบกพร่อง ไม่มีม้าม หรือม้ามทำงานผิดปกติ
3) เด็กภูมิคุ้มกันปกติอายุ 2 ปีขึ้นไปไม่จำเป็นต้องฉีด Hib
Polio Vaccine: IPV + OPV — Injectable vs Oral
IPV — Inactivated Polio Vaccine (ชนิดฉีด)
Inactivated Vaccine: Contains killed poliovirus Types 1, 2, and 3. Induces systemic humoral antibodies to prevent paralysis and Vaccine-associated paralytic poliomyelitis (VAPP).
Schedule: IPV at 2 and 4 months. Route and dose follow the licensed product and local administration guidance.
Interchangeability & Precautions
IPV can be given as a replacement for oral OPV drops at any visit to eliminate the risk of VAPP.
Contraindications: Severe anaphylaxis to a prior dose or known severe allergy to Neomycin, Streptomycin, or Polymyxin B.
OPV — Oral Polio Vaccine (ชนิดกิน)
Live-attenuated Vaccine: Bivalent formulation containing attenuated poliovirus Types 1 and 3. Induces robust local intestinal mucosal immunity (Secretory IgA) to block wild virus transmission.
Schedule: 2 drops orally at 6 months, 18 months, and 4–6 years of age (3 doses total).
Absolute Contraindications
Do not use OPV in: Immunodeficient patients, household contacts of immunodeficient individuals, or pregnant women. Use IPV exclusively for these groups.
Very rare risk of vaccine-associated paralytic polio (VAPP) in healthy individuals.
คำอธิบายเต็ม: โปลิโอ (IPV + OPV)
1) ให้ IPV 2 ครั้ง อายุ 2 และ 4 เดือน จากนั้น bivalent OPV ที่อายุ 6 เดือน, 18 เดือน และ 4–6 ปี
2) ใช้ IPV แทน OPV ได้ทุกครั้ง หากใช้ IPV อย่างเดียวตลอด อาจให้รวม 4 ครั้ง โดยงดเข็มอายุ 18 เดือนได้
Rotavirus Vaccine (Rota - Oral Administration)
Age Constraints & Dosing
Oral Live-attenuated Vaccine: Prevents severe watery diarrhea caused by Rotavirus, particularly in infants. Available as 2-dose (Rotarix) or 3-dose (RotaTeq) regimens.
Age limits: Follow the licensed product and current PIDST/WHO guidance. Keep doses at least 4 weeks apart and complete within the product age limit.
Contraindications & Spit-out Protocol
Contraindications: Documented history of Intussusception, Severe Combined Immunodeficiency (SCID), or severe allergic reactions to prior doses.
Spit-out Protocol: If the infant vomits or spits out the vaccine during administration, do not repeat the dose. Proceed with the routine schedule.
คำอธิบายเต็ม: โรตาไวรัส (Rotavirus)
1) Rotarix ให้รับประทาน 2 ครั้ง อายุ 2 และ 4 เดือน; Rotavac ให้ 3 ครั้ง อายุ 2, 4 และ 6 เดือน
2) RotaTeq หรือ Rotasil ให้รับประทาน 3 ครั้ง อายุ 2, 4 และ 6 เดือน
3) เริ่มเข็มแรกอายุ 6–15 สัปดาห์ เข็มสุดท้ายไม่เกิน 8 เดือน แต่ละครั้งห่างกันอย่างน้อย 4 สัปดาห์
4) ควรใช้วัคซีนชนิดเดียวกันจนครบ หากต่างชนิดหรือไม่ทราบชนิดเดิม ให้ครบ 3 ครั้ง
5) ให้ร่วมกับ OPV ได้
6) ห้ามใช้ใน SCID ผู้มีประวัติลำไส้กลืนกัน หรือแพ้วัคซีนรุนแรง
Measles, Mumps, Rubella Vaccine (MMR - Live Viral)
Mechanism & Target Schedule
Live-attenuated Vaccine: Induces immunity against Measles, Mumps, and Rubella to control outbreaks and prevent congenital rubella syndrome.
Schedule: 0.5 mL at 9–12 months and 18 months. Route and site follow the licensed product and local administration guidance.
Key Spacing & HIV Precautions
Maternal Antibody Waning: Early dose at 9 months is selected to protect infants as maternal antibodies fade, reducing the measles window of susceptibility.
Immunocompromised: Live MMR is contraindicated in severe immunosuppression. Assess HIV status using age-specific clinical and laboratory criteria.
คำอธิบายเต็ม: หัด–คางทูม–หัดเยอรมัน (MMR)
1) เข็มแรกอายุ 9–12 เดือน และเข็มที่ 2 อายุ 18 เดือน
2) หากระบาด: เริ่มได้ตั้งแต่อายุ 6 เดือน และฉีดซ้ำตามกำหนด; เริ่มอายุ 9–12 เดือน เว้นอย่างน้อย 3 เดือน; เริ่มหลัง 12 เดือน เว้นอย่างน้อย 1 เดือน
3) ควบคุมการระบาดอาจใช้ MR ในเด็กอายุมากกว่า 4 ปีและผู้ใหญ่
4) ใช้ MMRV แทน MMR และ VZV แยกเข็มได้ แต่เข็มแรกอายุ 12–47 เดือนมีความเสี่ยงไข้ชักสูงกว่า
5) หากเคย MMR หรือ VZV ให้ MMRV ห่างอย่างน้อย 3 เดือน
Japanese Encephalitis Vaccine (JE - Live SA14-14-2 vs. Inactivated)
Live-attenuated JE (LAJE)
SA14-14-2 Strain: Provided under NIP. Highly immunogenic with only 2 doses.
Timeline: 0.5 mL SC injection at deltoid. Dose 1 at 9–12 months; Dose 2 12–24 months later. Minimum interval depends on product: 3 months for CD-JEVAX; 12 months for IMOJEV/THAIJEV.
Inactivated JE (Vero Cell)
May be used when live JE is contraindicated, according to product-specific and PIDST guidance. Requires 3 doses: Dose 1 and 2 separated by 1-4 weeks starting at 6 months, and Dose 3 at 1 year.
Live Spacing Rule: Live injectables (MMR, LAJE, Varicella) must be given on the same day or separated by ≥ 28 days.
คำอธิบายเต็ม: ไข้สมองอักเสบเจอี (JE)
1) JEVAC ชนิดเชื้อตาย ฉีด 3 ครั้ง เริ่มอายุ 6 เดือน เข็มถัดไปห่าง 1–4 สัปดาห์ และเข็มที่ 3 อีก 1 ปี
2) Live JE ให้ 2 ครั้ง: เข็มแรก 9–12 เดือน และเข็มที่ 2 ห่าง 12–24 เดือนตามผลิตภัณฑ์
3) หากได้รับชนิดเชื้อตายไม่ครบ ให้ฉีดต่อด้วย live JE ตามจำนวนและระยะห่างที่แนะนำ ไม่ต้องเริ่มใหม่
Pneumococcal Conjugate Vaccine (PCV - New NIP Benefit 2026)
Indications & Clinical Impact
PCV Conjugate Formulation: Prevents invasive pneumococcal diseases (IPD) including sepsis, meningitis, and bacteremic pneumonia, as well as acute otitis media in infants.
Schedule: Standard PCV schedule is 2, 4, 6 months with a booster at 12–15 months; a 2+1 schedule (2, 4, and 12–15 months) may be used for healthy children according to current guidance.
PCV Catch-up Guidelines
Healthy Children < 5 years: If immunization is delayed, arrange catch-up doses until age 5. Dose count depends on initiation age.
Highly recommended for at-risk cohorts: children with asplenia, sickle cell disease, chronic lung/heart diseases, or immunocompromised states.
คำอธิบายเต็ม: นิวโมคอคคัส (PCV)
1) ให้ในเด็กเสี่ยงโรครุนแรงและเด็กปกติอายุน้อยกว่า 5 ปี
2) PCV10, PCV13, PCV14, PCV15 หรือ PCV20 ให้ 3 ครั้ง อายุ 2, 4, 6 เดือน และกระตุ้น 12–15 เดือน ห่างเข็มสุดท้ายอย่างน้อย 2 เดือน
3) เด็กปกติอาจใช้ตาราง 2+1: อายุ 2, 4 และ 12–15 เดือน
4) พิจารณา catch-up ในเด็กอายุน้อยกว่า 5 ปีที่ยังไม่เคยได้ PCV
เด็กเสี่ยง ได้แก่ ภูมิคุ้มกันบกพร่อง ไม่มีม้าม โรคปอด หัวใจ ตับ ไต เบาหวาน หรือ CSF leak/cochlear implantation
HPV Vaccine (Human Papillomavirus - Cervical Cancer Prevention)
Schedules by Age Group
Human Papillomavirus Recombinant Vaccine: Prevents HPV infection and HPV-associated precancers and diseases, including genital warts; cancer-endpoint wording depends on product and guideline context.
Ages 9-14 years: 2 doses (IM) separated by 6-12 months.
Ages ≥ 15 years: 3 doses (IM) at 0, 1-2, and 6 months.
School-Based Campaigns (Grade 5)
National school immunization targets Grade 5 girls (approx 11-12 years). Provided free under NIP. For healthy persons aged 9–20 years, WHO 2022 allows a one-dose option; immunocompromised persons should receive at least 2 doses, preferably 3. Do not vaccinate during pregnancy; complete remaining doses after pregnancy.
คำอธิบายเต็ม: เอชพีวี (HPV)
1) มีชนิด 2, 4 และ 9 สายพันธุ์; หากต้องการป้องกันหูดหงอนไก่ใช้ชนิด 4 หรือ 9 สายพันธุ์
2) แนะนำหญิงและชายอายุ 9–26 ปี โดยเน้นอายุ 11–12 ปี; ตาราง 3 เข็มที่เดือน 0, 1–2 และ 6
3) วัยรุ่นแข็งแรงที่เริ่มก่อนอายุ 15 ปี ใช้ 2 เข็มที่ 0 และ 6–12 เดือน
4) อายุ 9 ปีขึ้นไปอาจใช้ 2 เข็มห่างอย่างน้อย 6 เดือน; ผู้มีภูมิคุ้มกันบกพร่องควรได้อย่างน้อย 2 เข็ม และถ้าเป็นไปได้ 3 เข็ม
5) แผนกระทรวงฯ ให้ HPV9 1 เข็มแก่เด็กหญิง ป.5 หรืออายุ 11–12 ปี; หากไม่มี HPV9 ใช้ชนิด 2 หรือ 4 สายพันธุ์ 2 เข็มห่างอย่างน้อย 6 เดือน
6) เปลี่ยนจากชนิด 2/4 เป็นชนิด 9 เพื่อให้ครบได้ และหากครบแล้วไม่จำเป็นต้องฉีดเพิ่ม
dT Vaccine (Diphtheria-Tetanus Booster)
School Boosters & Adults
dT Toxoid Vaccine: Replaced tetanus toxoid (TT) alone in school campaigns to maintain population herd immunity against Diphtheria.
School Program (Grade 6): 1 dose IM at deltoid (approx 12 years of age).
Adult routine: Use dT every 10 years according to local guidance; use Tdap for at least one lifetime booster when indicated.
Clinical Prophylaxis in Trauma
For dirty or major wounds, give a booster when indicated if the primary series is complete and the last dose was ≥5 years ago. If history is incomplete or unknown, assess for a primary series and tetanus immune globulin (TIG) according to wound guidance.
คำอธิบายเต็ม: dT / Tdap
เด็กอายุ 11–12 ปีควรได้รับ Td, Tdap หรือ TdaP ไม่ว่าจะเคยได้รับตอน 4–6 ปีหรือไม่ หลังจากนั้นกระตุ้นทุก 10 ปี
หญิงตั้งครรภ์ควรได้รับ aP/Tdap 1 เข็มทุกการตั้งครรภ์ อายุครรภ์ 20–32 สัปดาห์ เพื่อถ่ายทอดภูมิไปยังทารก
EPI Catch-up Guidelines (Delayed Vaccination)
Core Principles
- Do Not Restart: If a child misses a scheduled dose, resume the series. Do not restart the series.
- Minimum intervals: Use vaccine-specific minimum intervals; 4 weeks applies only to selected dose gaps.
- Age limits: Routine start is 6–15 weeks and final dose by 8 months; selected older infants may be considered up to age 2 years after risk–benefit discussion under PIDST/WHO guidance.
Clinical Scenario: Delayed 1-Year-Old
For a 1-year-old child presenting with only BCG and HepB1 at birth:
Absolute Contraindications vs. Misconceptions
Absolute Contraindications (Do Not Vaccinate)
False Contraindications (Safe to Vaccinate)
Common misconceptions that lead to unnecessary vaccine delays (Missed Opportunities). Immunization is safe during:
Adverse Events Following Immunization (AEFI) & Anaphylaxis Management
Common Reactogenicity
Fever & local pain: Common after DTPw. Use paracetamol for symptomatic relief according to age, weight, maximum daily dose, and local protocol; do not routinely premedicate.
BCG local reaction: Explain expected healing and keep the site clean. Routine uncomplicated lesions do not require aspiration; refer fluctuant or suppurative lymphadenitis for specialist assessment.
Emergency Response: Anaphylaxis Protocol
All immunization clinics must have a fully stocked Anaphylaxis Emergency Kit and trained staff.
References
Vancouver style
- Pediatric Infectious Disease Society of Thailand. ตารางการสร้างเสริมภูมิคุ้มกันโรคในเด็กและวัยรุ่นไทย แนะนำโดย สมาคมโรคติดเชื้อในเด็กแห่งประเทศไทย 2569 [Internet]. Bangkok: PIDST; 2026 Feb 3 [cited 2026 Jul 19]. Available from: https://www.pidst.or.th/A1627.html
- Department of Disease Control, Ministry of Public Health, Thailand. National immunization program schedule: Thailand 2026 [Internet]. Nonthaburi: Department of Disease Control; 2026 [cited 2026 Jul 19].
- World Health Organization. Human papillomavirus vaccines: WHO position paper, December 2022. Wkly Epidemiol Rec. 2022;97(50):645-672.
- World Health Organization. Influenza vaccines: WHO position paper, May 2022. Wkly Epidemiol Rec. 2022;97(19):185-208.
- World Health Organization. Rotavirus vaccines: WHO position paper—January 2013. Wkly Epidemiol Rec. 2013;88(5):49-64.
- World Health Organization. Pneumococcal conjugate vaccines in infants and children under 5 years of age: WHO position paper—February 2019. Wkly Epidemiol Rec. 2019;94(8):85-104.
- World Health Organization. Japanese encephalitis vaccines: WHO position paper—February 2015. Wkly Epidemiol Rec. 2015;90(9):69-88.
- World Health Organization. Measles vaccines: WHO position paper—April 2017. Wkly Epidemiol Rec. 2017;92(17):205-228.
- World Health Organization. BCG vaccines: WHO position paper—February 2018. Wkly Epidemiol Rec. 2018;93(8):73-96.
- World Health Organization. Hepatitis B vaccines: WHO position paper—July 2017. Wkly Epidemiol Rec. 2017;92(27):369-392.
Accessed 19 July 2026. Local source file: 000Tarang Feb5VX2026.pdf, p. 2.
คำอธิบายวัคซีน — PIDST 2569 หน้า 2 ต้นฉบับ
หน้าอ้างอิงเต็มจาก PDF ไม่ตัดคำ สามารถเปิดภาพในแท็บใหม่เพื่อขยาย